Head Shape Deformities in Babies

By Sarah Russell
Since placing babies on their backs to sleep was introduced through the ‘Safe to Sleep’ (1) initiative, positional head shape deformities have become more common (2).
What is positional head shape deformity?
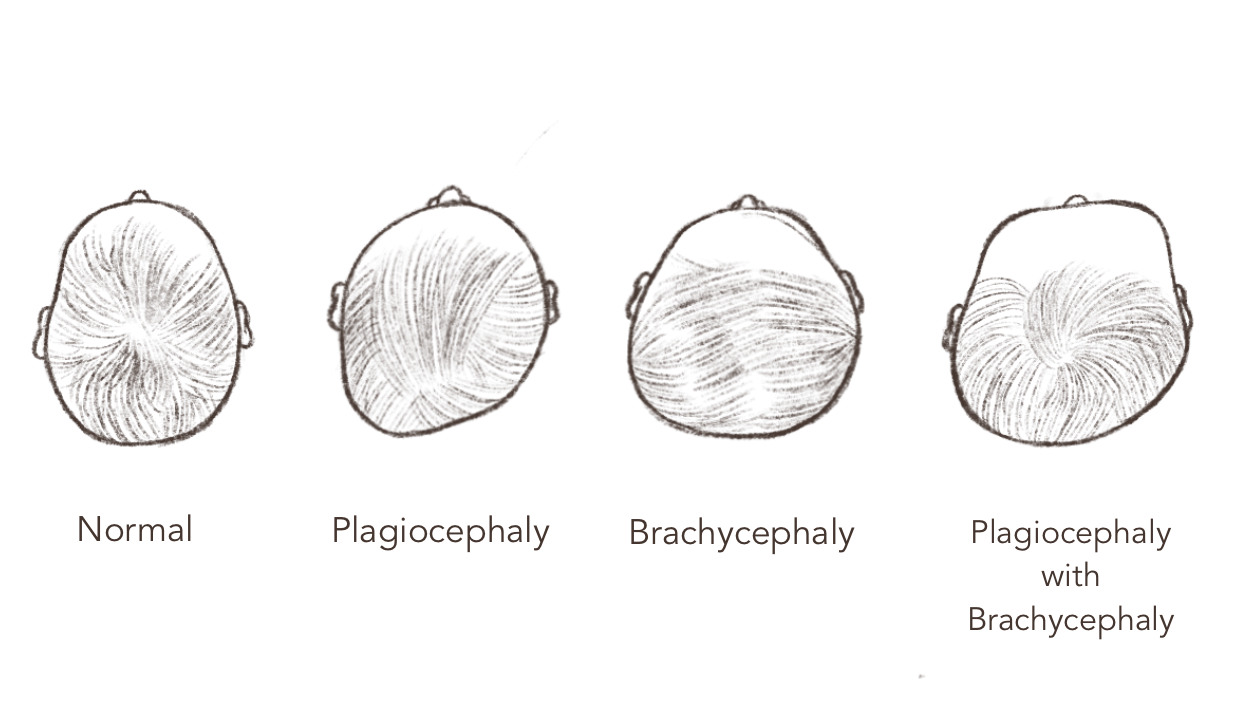
Positional head shape deformities (PHD) are one subtype of the group of conditions that make up what is commonly known as ‘flat head syndrome.’ The term ‘positional head shape deformity’ refers to a “misshapen, flat or asymmetrical (uneven) head shape” (3) which develops as a result of a baby spending a significant amount of time on their backs in the same position. PHD may be categorized as either positional plagiocephaly or positional brachycephaly (or a combination of both). The location of the flatness will dictate the type of positional head shape deformity, as detailed in figure 1.
What causes PHD?
Positional head shape deformities are reported to affect 30% of babies throughout the first year of life (4) with most cases presenting in the first few months (5) up until the first six months of life (6). Prolonged compressive forces on the soft, malleable, and rapidly growing skull—often as a result of babies spending a significant amount of time on their backs in the same position, either throughout the day or at any one time—can result in positional head shape deformities (7). However, the condition may also be related to a variety of other contributing factors (8) such as:
- Male sex
- First born
- Assisted delivery
- Neck stiffness (e.g., torticollis)
How do I know if my baby has a head shape deformity?
Babies with head shape deformities will present with one or a combination of the following and it is the significance of these factors that will contribute to the extent of the deformity:
- A flattened area across the back and/or side of the head (from a bird’s eye view you may notice your baby’s head shape isn’t round but rather slanted in a certain area)
- Head may appear wide from above the ears when looking at your baby from in front of them
- Ear displacement (ears may be misaligned and may protrude)
- Forehead protrusion
- Bony prominences near the ears, close to the temples
Because babies are most at risk, it is important to be aware of positional head shape deformities. Hence parents are encouraged to pay close attention to their baby’s head shape.
The most accurate way to look at your baby’s head shape is when their hair is wet (if they have a lot of hair), or if your baby hasn’t a lot of hair, you should be able to make an assessment irrespective of their hair being wet. A bird’s eye view of their head will help you identify any abnormalities along with looking at the head from side-on (both left and right sides). It is recommended that you look at your baby’s head shape weekly in the event flat spots are developing.
What can I do?
Here are some general recommendations that may help if you notice changes to your baby’s head shape:
- Ensure you play with your baby in various positions (e.g., on their back, tummy, and sides). Your baby will still benefit from playing on their back during wake periods, irrespective of any flat spots, but varying their position for play is beneficial for reducing pressure off the back of the skull.
- Encourage your baby to turn their head left and right to look, interact, and play with you by keeping in mind which side you approach them from, and where you sit to play with them. Also, when you choose a place to play, consider on which side items of interest are (e.g., window, entrance to a room).
- Remove any pillows from your baby’s sleep environment. An infant pillow or any other pillow/head support can—and often does—restrict your baby’s ability to move their head, making them susceptible to PHD, especially if they have any neck stiffness. Importantly, pillows and other positioning supports are not encouraged in the safe sleep guidelines (9).
- During sleep times, alternate the side you place your baby in their sleeping space to sleep so that their head is facing into the room. This means that you will be positioning your baby at opposite ends of the crib each time they go to sleep.
Therapist tip: wear an elastic band on your wrist to help you remember which side to place them on for sleep.
- Remove any overhead play gyms, which typically encourage your baby to keep their head in a static position. Instead, try positioning toys to both sides of your baby to encourage them to move their head and neck.
- Use a baby carrier. Ensure you alternate the side of the head that is resting on your chest, particularly if your baby is not yet able to move their head fully.
- Limit time in bouncers, baby loungers, and support pillows.
- Vary the way you hold your baby and the arm you use to carry, rock them to sleep, and feed them (if bottle feeding).
Take home points from an occupational therapy perspective
- If you notice any changes to your baby’s head shape, have concerns about your baby’s ability to move their head from side to side, or you notice your baby has a strong preference for turning their head to one side, please contact a pediatric occupational therapist, or a physiotherapist or pediatrician with expertise in managing head shape deformities.
- If your baby has a flat spot developing on their head, it is important to seek support as soon as possible. Positional head shape deformities have been associated with developmental delays. Early detection and prompt treatment may improve motor development (10).
- Despite any head shape deformities, you should still sleep your baby on their back in accordance with the ‘Safe to Sleep’ guidelines (11).
- There are a variety of interventions that can be implemented to help reduce the severity of head shape deformities. These can include repositioning and handling recommendations and specific strengthening and stretching activities. A custom made helmet to reshape the head may also need to be considered. This will depend on the severity of the PHD and also take into account the age at which the PHD is detected.
- Babies should experience a variety of play positions other than lying on their back while they are awake and supervised.
References
1) Safe To Sleep. (2021) Ways to reduce the risk of SIDS and other sleep-related causes of infant death. safetosleep.nichd.nih.gov/safesleepbasics/risk/reduce
2) Hutchison BL et al. (2010) A randomised controlled trial of positioning treatments in infants with deformational plagiocephaly. Acta Paediatrica, 99, 1556–1560. pubmed.ncbi.nlm.nih.gov/20491708/;
3) The Royal Children’s Hospital. (2020) Kids Health Information: Plagiocephaly – misshapen head. rch.org.au/kidsinfo/fact_sheets/Plagiocephaly_misshapen_head/
4) See ref. 2
5) Bialocerkowski AE et al. (2008) Prevalence, risk factors, and natural history of positional plagiocephaly: a systematic review. Developmental Medicine and Child Neurology, 50, 577–86. pubmed.ncbi.nlm.nih.gov/18754894/
6) Hutchison BL et al. (2004) Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study. Paediatrics, 114, 970–80. pubmed.ncbi.nlm.nih.gov/15466093/
7) Hutchison, BL et al. (2011) Deformational Plagiocephaly: A follow- up of head shape, parental concern and neurodevelopment at ages 3 and 4 years. Archive of Disease in Childhood, 96, 85–90. adc.bmj.com/content/96/1/85
8) See ref. 5
9) See ref. 1
10) Martiniuk, A. L. C. et al. (2017). Plagiocephaly and Developmental Delay: A Systematic Review. Journal of Developmental and Behavioural Pediatrics, 38, 67-78. ingentaconnect.com/content/wk/dbp/2017/00000038/00000001/art00012
11) See ref. 1
Further Reading
Gonzales-Santos, J., Gonzales-Bernal, J., De-la-Fuente-Anuncibay, R., et al (2020). A Prospective Study of Cranial Deformity and Delayed Development in Children. Sustainability, 12, 1949-1957.
Photos from Canva.
About the Author
Sarah Russell is an Australian-trained pediatric occupational therapist with expertise in head shape deformities. Since 2014, Sarah has been working in South East Asia, formerly in an international school and private practice, until becoming a mum herself. Sarah is particularly interested in empowering babies to move, grow, and thrive through simple, yet fun and interactive play. To contact Sarah, please email: stamburrini@gmail.com